BMA Presentations 16 Jan 2018
|
https://bma.public-i.tv/core/portal/webcast_interactive/316306 |


World Association for Cultural Psychiatry, Mexico 2015

Stigma, conflict and group identity
Dr N Yoganathan
As human beings began to live in groups, they inevitably created hierarchies to maintain order. Social strata (e.g. caste, class) were incorporated as culture with beliefs and practices becoming normalised and even dogmatised. History records how this led to crusades, civil wars, slave trade etc. Enlightenment, scientific discoveries and industrial revolution brought some levelling of the hierarchy but did not prevent revolutions, due to the gap between the ‘haves’ and ‘havenots’. Abolition of slavery and the growth of democracy created an illusion that we could live in harmony but two world wars shattered this dream. Post WW2 saw an artificial balance between two ideologies (capitalists vs socialist/communist) resulting in the Cold War, which gave a false sense of stability. But the growth of a market economy model and the collapse of the socialistic model, with unchecked capitalism, has further widened the inequality. Isn’t it inevitable, that this medium is fertile for the growth of even more radical ideologies, based on some romantic and idealised view of the past? Proponents use the very elements of stigmatisation (ignorance, isolation, victimisation) to recruit more followers through monologue and duologue. These destructive group phenomena (envy, splitting, projection) can only be reversed through a constructive group process. To deal with this we must confront our own prejudices in order to reverse the cycle: contact, education, acceptance will empower individuals rather than let them be seduced by fanatical ideology. This requires a compassionate approach based on openness, dialogue, tolerance and empathy by all parties concerned.
Dr N Yoganathan
As human beings began to live in groups, they inevitably created hierarchies to maintain order. Social strata (e.g. caste, class) were incorporated as culture with beliefs and practices becoming normalised and even dogmatised. History records how this led to crusades, civil wars, slave trade etc. Enlightenment, scientific discoveries and industrial revolution brought some levelling of the hierarchy but did not prevent revolutions, due to the gap between the ‘haves’ and ‘havenots’. Abolition of slavery and the growth of democracy created an illusion that we could live in harmony but two world wars shattered this dream. Post WW2 saw an artificial balance between two ideologies (capitalists vs socialist/communist) resulting in the Cold War, which gave a false sense of stability. But the growth of a market economy model and the collapse of the socialistic model, with unchecked capitalism, has further widened the inequality. Isn’t it inevitable, that this medium is fertile for the growth of even more radical ideologies, based on some romantic and idealised view of the past? Proponents use the very elements of stigmatisation (ignorance, isolation, victimisation) to recruit more followers through monologue and duologue. These destructive group phenomena (envy, splitting, projection) can only be reversed through a constructive group process. To deal with this we must confront our own prejudices in order to reverse the cycle: contact, education, acceptance will empower individuals rather than let them be seduced by fanatical ideology. This requires a compassionate approach based on openness, dialogue, tolerance and empathy by all parties concerned.
Wellbeing & Global Mental Health
Dr Jenny Willis
Wellbeing, whilst not a panacea for mental health, can be important to the defence against and recovery from mental illnesses. For over a decade, the Organisation for Economic Co-operation and Development has been measuring and comparing perceptions of wellbeing based on life-evaluation, affect and eudaimonia (self-actualisation). The United Nations Children’s Fund report, Child Wellbeing in Rich Countries (Innocenti Report Card 11, 2013) compares children’s wellbeing nationally according to five dimensions: wealth; health and safety; education; behaviour and risks, and housing and environment. The significance of such work is that it recognises the centrality of personal needs and social contexts to our sense of wellbeing. In 2011, the UK Department of Health launched its strategy ‘No Health Without Mental Health: A Cross-Government Mental Health Outcomes Strategy for People of All Ages’. Despite references to inequality and enabling individuals to take personal control of their lives, this strategy was clearly driven by financial imperatives: mental illness (unwellbeing) makes serious demands on the national economy. In response, the national economic foundation (nef) identified a set of measurable indicators, 5 Ways to Wellbeing (2010) designed to maximise wellbeing by making ‘healthy’ lifestyle choices, drawing from a menu of five domains: connecting with others; being active; taking notice; keeping on learning; and giving to others. My comparative research with groups in the UK, China and Argentina highlighted the variability of conceptions according to cultural norms. Participants are invited to complete a similar questionnaire so that we can explore common features of wellbeing.
Dr Jenny Willis
Wellbeing, whilst not a panacea for mental health, can be important to the defence against and recovery from mental illnesses. For over a decade, the Organisation for Economic Co-operation and Development has been measuring and comparing perceptions of wellbeing based on life-evaluation, affect and eudaimonia (self-actualisation). The United Nations Children’s Fund report, Child Wellbeing in Rich Countries (Innocenti Report Card 11, 2013) compares children’s wellbeing nationally according to five dimensions: wealth; health and safety; education; behaviour and risks, and housing and environment. The significance of such work is that it recognises the centrality of personal needs and social contexts to our sense of wellbeing. In 2011, the UK Department of Health launched its strategy ‘No Health Without Mental Health: A Cross-Government Mental Health Outcomes Strategy for People of All Ages’. Despite references to inequality and enabling individuals to take personal control of their lives, this strategy was clearly driven by financial imperatives: mental illness (unwellbeing) makes serious demands on the national economy. In response, the national economic foundation (nef) identified a set of measurable indicators, 5 Ways to Wellbeing (2010) designed to maximise wellbeing by making ‘healthy’ lifestyle choices, drawing from a menu of five domains: connecting with others; being active; taking notice; keeping on learning; and giving to others. My comparative research with groups in the UK, China and Argentina highlighted the variability of conceptions according to cultural norms. Participants are invited to complete a similar questionnaire so that we can explore common features of wellbeing.
Stigma, Empowerment and Mental Health, November 2013

In November 2013, we had the pleasure of leading a 2-hour workshop at the Ministry of Finance, London, Ontario.
This was an interactive session, divided into two complementary parts: 1. Stigma and mental illness; 2. Personal Wellbeing.
The report of these sessions is attached below.
This was an interactive session, divided into two complementary parts: 1. Stigma and mental illness; 2. Personal Wellbeing.
The report of these sessions is attached below.
See the report for exciting comparative data across 4 cultures
| toronto_report_november_2013.pdf |
Stigma, dementia and mental illness, September 2013
| madness_of_psychiatry_feedback_august_2013.pdf |
| sept_2013.xps |
| stigma_and_dementia_feedback_16.09.13.pdf |
Argentina Wellbeing Survey August 2013
| summary_wellbeing_survey_argentina_2013.pdf |
ARGENTINA August 2013
For a copy of our presentations, The Madness of Psychiatry in 21st century UK or Confronting stigma: wellbeing not illbeing, please email us at [email protected] and we will send you the file.
INTERNATIONAL EVENTS
WORLD FEDERATION FOR MENTAL HEALTH, Buenos Aires August 2013
THE MADNESS OF PSYCHIATRY (in the 21st Century UK) A GROUP ANALYTIC PERSPECTIVE
Dr N Yoganathan
Over 2½centuries, 100 asylums were built to manage some 150,000 mentally/socially ‘insane’. Socio-political ideologies closed these institutions in 50 years but merely displaced more patients/residents/inmates to community/hospital/prison settings, despite much-improved treatments and staffing.
Society’s anxieties/stigma are contained by metaphorical chains/straightjackets: policies, guidelines, assessments (risk), licenses (medications) and penal/legal rituals.
‘Mindless efficiency targets/(dys)functional, politically-correct models’, have led to staff/services being split, becoming ‘psychotically’ anxious, grandiose, paranoid and emotionally incongruent/ambivalent, resembling 'schizophrenia'.
The art of intuitive therapy/care is increasingly replaced by impersonal/thoughtless obsessive/compulsive, ‘quasi-evidence-based/magical(undoing)’ tick-box psychiatry.
In the ’80s it was ‘Community Care’; ‘90s ‘Community Scare’; ‘00s ‘Community Chaos’; now ‘Community Scarce’.
Dr N Yoganathan
Over 2½centuries, 100 asylums were built to manage some 150,000 mentally/socially ‘insane’. Socio-political ideologies closed these institutions in 50 years but merely displaced more patients/residents/inmates to community/hospital/prison settings, despite much-improved treatments and staffing.
Society’s anxieties/stigma are contained by metaphorical chains/straightjackets: policies, guidelines, assessments (risk), licenses (medications) and penal/legal rituals.
‘Mindless efficiency targets/(dys)functional, politically-correct models’, have led to staff/services being split, becoming ‘psychotically’ anxious, grandiose, paranoid and emotionally incongruent/ambivalent, resembling 'schizophrenia'.
The art of intuitive therapy/care is increasingly replaced by impersonal/thoughtless obsessive/compulsive, ‘quasi-evidence-based/magical(undoing)’ tick-box psychiatry.
In the ’80s it was ‘Community Care’; ‘90s ‘Community Scare’; ‘00s ‘Community Chaos’; now ‘Community Scarce’.

Bethlem Hospital, London
CONFRONTING STIGMA: WELLBEING NOT ILLBEING
Dr Jenny Willis

The UK’s 2011 strategy No Health without Mental Health led to 5 Ways to Wellbeing, a set of 5 contributors (connect/be active/take notice/keep learning/give) aimed at enhancing wellbeing and preventing mental ill-health by incorporating activities related to the 5 factors in our everyday lives. The Lifewide Education Community champions similar dimensions through our drive for lifewide learning. This interactive workshop will present the findings of our small-scale survey conducted in 2013 on perceptions of wellbeing in the UK and Beijing. We will conduct the same survey with participants and present the results in our campaign to destigmatise mental illness.
Gamian-Europe Keynote Speech Zagreb November 2007
STIGMA AND EMPOWERMENT
Dr N Yoganathan, with Dr J Willis
As human beings, our greatness lies not so much in being able to remake the world - that is the myth of the atomic age - as in being able to remake ourselves Mohandas Gandhi
This keynote speech will include an interactive session, offering the audience an opportunity to participate in the dynamic process proposed by the speakers. Participants will be prompted to complete sections of a questionnaire during the presentation. Responses will later be collated and fed back to participants.
As a doctor who trained in psychiatry in the 1980s, and having worked as a Consultant Psychiatrist in the public and private sectors in the UK, Dr Yoganathan will begin by describing some of the major changes in mental health provision in England over the last two decades. He will then hand over to Dr Willis, who will look at recent models of stigma, both in mental illness and in general, and at ways of addressing stigmatisation.
Dr Yoganthan will resume his presentation. He will consider concepts of health and ill health and the role of stigma. He will argue that stigma is an inevitable product of group living. It is natural for groups to become exclusive, creating local rules, leading to the formation of hierarchies. Individuals who do not conform to such rules may also exclude themselves, unconsciously contributing to further stigmatisation. This didactic process derives from primitive emotions, which are evoked when we are confronted by ambivalent situations. It is understandable that stigma associated with mental illness is often attributed to society’s lack of empathy and comprehension, but, to effect change at this level, may take generations.
Instead, the speakers argue that empowerment is more achievable if we address stigma at a personal level. Before we can experience true empowerment, we must acknowledge our own ambivalence towards stigmatisation. Recognition of this ambivalence within ourselves is the first step towards confronting anxieties and negotiating the grieving process inevitable for healing to take place. To achieve this, we must be open and dialectical in our thinking, making way for healthier dialogue within ourselves and with others.
“For successful rehabilitation in psychiatry, we need to address the anxieties first of staff, then of relatives/carers and finally patients.”
Yoganathan, N. 2007 WFMH Congress, ‘Zen, Stigma and Mental Health
Dr N Yoganathan, with Dr J Willis
As human beings, our greatness lies not so much in being able to remake the world - that is the myth of the atomic age - as in being able to remake ourselves Mohandas Gandhi
This keynote speech will include an interactive session, offering the audience an opportunity to participate in the dynamic process proposed by the speakers. Participants will be prompted to complete sections of a questionnaire during the presentation. Responses will later be collated and fed back to participants.
As a doctor who trained in psychiatry in the 1980s, and having worked as a Consultant Psychiatrist in the public and private sectors in the UK, Dr Yoganathan will begin by describing some of the major changes in mental health provision in England over the last two decades. He will then hand over to Dr Willis, who will look at recent models of stigma, both in mental illness and in general, and at ways of addressing stigmatisation.
Dr Yoganthan will resume his presentation. He will consider concepts of health and ill health and the role of stigma. He will argue that stigma is an inevitable product of group living. It is natural for groups to become exclusive, creating local rules, leading to the formation of hierarchies. Individuals who do not conform to such rules may also exclude themselves, unconsciously contributing to further stigmatisation. This didactic process derives from primitive emotions, which are evoked when we are confronted by ambivalent situations. It is understandable that stigma associated with mental illness is often attributed to society’s lack of empathy and comprehension, but, to effect change at this level, may take generations.
Instead, the speakers argue that empowerment is more achievable if we address stigma at a personal level. Before we can experience true empowerment, we must acknowledge our own ambivalence towards stigmatisation. Recognition of this ambivalence within ourselves is the first step towards confronting anxieties and negotiating the grieving process inevitable for healing to take place. To achieve this, we must be open and dialectical in our thinking, making way for healthier dialogue within ourselves and with others.
“For successful rehabilitation in psychiatry, we need to address the anxieties first of staff, then of relatives/carers and finally patients.”
Yoganathan, N. 2007 WFMH Congress, ‘Zen, Stigma and Mental Health
Related paper

www.gamian.eu/newsletters/ge_newsletter27.pdf
File Format: PDF/Adobe Acrobat - Quick View
4 Jul 2007 – Year 9, no 27, autumn winter 2007 ... over the last year in activities which. GAMIAN .... CONVENTION Report on the X GAMIAN Europe. 2007 ...
File Format: PDF/Adobe Acrobat - Quick View
4 Jul 2007 – Year 9, no 27, autumn winter 2007 ... over the last year in activities which. GAMIAN .... CONVENTION Report on the X GAMIAN Europe. 2007 ...
World Federation for Mental Health, East meets West, Hong Kong August 2007
ZEN, STIGMA, MENTAL HEALTH & MENTAL ILLNESS: A clash of nature and culture (professional, political, economic and scientific environment)
Dr N Yoganathan
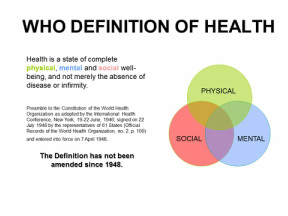
‘It is more important to know what sort of person has a disease than to know what sort of a disease a person has.’ Hippocrates (c. 460 BC - 377 BC)
Mental illnesses tend to alienate individuals from society (large group). This is essential for mutual existence. Any treatment and rehabilitation which does not aim to reintegrate the individual into wider society is doomed to fail in the long term. Median Groups offer a medium in which the anxieties of carers and patients can be managed more effectively. A process of dialogue encourages impersonal fellowship, helping individuals to discover and accept their own nature (Zen). This in turn aids destigmatisation, healing and recovery.
Since the 1970s, the UK has seen a socio-cultural change in psychiatric care provision, with closure of large asylums. Conversely, there has been an exponential increase in beds in low- and medium-secure settings, as well as a disproportionate rise in psychiatric morbidity in prisons (over 60% of inmates).
The recent mantra of Western clinical work is ‘evidence-based’ practice. While it may be justified for costly medical treatments to be objective, in psychiatry, this has led to CBT being used as a panacea. This and other quasi-scientific approaches and therapies undermine intuitive/interactive clinical practice, its spontaneity, humaneness and potential for healing.
Like the complementarity of Yin and Yang, provision of psychiatric care should integrate evidence- and tradition-based (culture) practices. This can only be achieved successfully through a process of dialogue (dialectic) between different agencies. Failure leads to didactic and divisive practices, resulting in further stigmatisation and alienation, as witnessed in the UK.
My eclectic practice, combining prescription and exploration (Median Groups), has demonstrated the paradox that, for successful rehabilitation in psychiatry, we need to address the anxieties first of staff, then of relatives/carers and finally patients.
Dr N Yoganathan
‘It is more important to know what sort of person has a disease than to know what sort of a disease a person has.’ Hippocrates (c. 460 BC - 377 BC)
Mental illnesses tend to alienate individuals from society (large group). This is essential for mutual existence. Any treatment and rehabilitation which does not aim to reintegrate the individual into wider society is doomed to fail in the long term. Median Groups offer a medium in which the anxieties of carers and patients can be managed more effectively. A process of dialogue encourages impersonal fellowship, helping individuals to discover and accept their own nature (Zen). This in turn aids destigmatisation, healing and recovery.
Since the 1970s, the UK has seen a socio-cultural change in psychiatric care provision, with closure of large asylums. Conversely, there has been an exponential increase in beds in low- and medium-secure settings, as well as a disproportionate rise in psychiatric morbidity in prisons (over 60% of inmates).
The recent mantra of Western clinical work is ‘evidence-based’ practice. While it may be justified for costly medical treatments to be objective, in psychiatry, this has led to CBT being used as a panacea. This and other quasi-scientific approaches and therapies undermine intuitive/interactive clinical practice, its spontaneity, humaneness and potential for healing.
Like the complementarity of Yin and Yang, provision of psychiatric care should integrate evidence- and tradition-based (culture) practices. This can only be achieved successfully through a process of dialogue (dialectic) between different agencies. Failure leads to didactic and divisive practices, resulting in further stigmatisation and alienation, as witnessed in the UK.
My eclectic practice, combining prescription and exploration (Median Groups), has demonstrated the paradox that, for successful rehabilitation in psychiatry, we need to address the anxieties first of staff, then of relatives/carers and finally patients.
World Federation for Mental Health, Hong Kong August 2007
Stigma and mental illness: challenging individual perceptions and measuring change
Dr Jenny Willis
In both mental health and education, traditional practice has been exclusive: the mentally ill have been confined, and access to forms of education has been restricted to those possessing a particular form of capital (financial, intellectual, class etc.) Whilst such systems have the advantage of being clearly defined, they are hierarchical, hence inequitable.
Modern technologies have broken down former boundaries, enabling access to what was once exclusive and creating a ‘global village,’ in a process that challenges and changes traditional values and practices. We no longer confine (exclude) those with a mental ‘illness’, but lack of confinement and integration within the community are not synonymous. So long as mental illness bears the imprint of stigma, the mentally ‘ill’ will remain apart.
Stigma is usually attributed to ‘society’ but society is no more than a collection of individuals, each of whom holds personal and collective beliefs and values. An individual’s beliefs become distinct if they differ from those of the collective: stigmatisation is thus a product of group processes. Challenging collectively held values, beliefs and stereotypes risks alienation and ostracism from the group (symbolic or actual death), hence effecting change in community values can take centuries.
A national 5-year campaign by the UK’s Royal College of Psychiatrists designed to challenge public perceptions of mental illness had disappointing results. We believe that that the first step in dealing effectively with stigma is to facilitate individuals to confront their own beliefs and assumptions. It is through the cumulative effect of individual change that we can best bring about sustainable and harmonious social change.
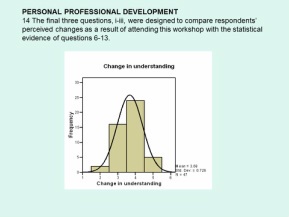
We demonstrate a small-scale study of how the impact of workshops on stigma in mental health delivered by a practising psychiatrist over the last three years has been evaluated, providing a model for refinement and wider application.
Dr Jenny Willis
In both mental health and education, traditional practice has been exclusive: the mentally ill have been confined, and access to forms of education has been restricted to those possessing a particular form of capital (financial, intellectual, class etc.) Whilst such systems have the advantage of being clearly defined, they are hierarchical, hence inequitable.
Modern technologies have broken down former boundaries, enabling access to what was once exclusive and creating a ‘global village,’ in a process that challenges and changes traditional values and practices. We no longer confine (exclude) those with a mental ‘illness’, but lack of confinement and integration within the community are not synonymous. So long as mental illness bears the imprint of stigma, the mentally ‘ill’ will remain apart.
Stigma is usually attributed to ‘society’ but society is no more than a collection of individuals, each of whom holds personal and collective beliefs and values. An individual’s beliefs become distinct if they differ from those of the collective: stigmatisation is thus a product of group processes. Challenging collectively held values, beliefs and stereotypes risks alienation and ostracism from the group (symbolic or actual death), hence effecting change in community values can take centuries.
A national 5-year campaign by the UK’s Royal College of Psychiatrists designed to challenge public perceptions of mental illness had disappointing results. We believe that that the first step in dealing effectively with stigma is to facilitate individuals to confront their own beliefs and assumptions. It is through the cumulative effect of individual change that we can best bring about sustainable and harmonious social change.
We demonstrate a small-scale study of how the impact of workshops on stigma in mental health delivered by a practising psychiatrist over the last three years has been evaluated, providing a model for refinement and wider application.
Related journal

www.onourownmd.org/wp-content/.../OOOMD-2011-Fall-web1.pdf
File Format: PDF/Adobe Acrobat - Quick View
Full Swing for Fall 2011 & ... and Medicaid Services (CMS) awarded PA a Systems. 1. 8. 9. 10. 11. 14. 16. 17 ... Consumer Network News ◇ Volume 18, Number 3 ◇ Autumn 2011 ...... Terry Bohrer, Diane Cabot, & Diane McComb, June 2007 ...
File Format: PDF/Adobe Acrobat - Quick View
Full Swing for Fall 2011 & ... and Medicaid Services (CMS) awarded PA a Systems. 1. 8. 9. 10. 11. 14. 16. 17 ... Consumer Network News ◇ Volume 18, Number 3 ◇ Autumn 2011 ...... Terry Bohrer, Diane Cabot, & Diane McComb, June 2007 ...
World Congress of the World Federation for Mental Health, Athens September 2009

Diaolgue: From Socrates to Darwin and Beyond (an experiential workshop/group)
Yoganathan, N. Dr. Convenor of Median Groups, Group Analytic Society, London;
Consultant Psychiatrist, St Mary’s Hospital, Isle of Wight PCT NHS Trust
[email protected]; [email protected]
Human beings have survived millennia with diverse perceptions of mental illness: from imbalance in humidity of the brain (Hippocrates) or of the humours (Galen), through religious or evil possession, to the socio-dynamics of asylums, psycho-dynamics (structure of the mind) and latterly neuro-psycho-pharmacological and cognitive/behavioural understanding (function of the mind).
Economic-socio-political ideals have led to closure of large asylums in most of the industrialised nations. Although these changes have brought more humane, and more scientifically measurable, treatments, a large number of vulnerable, mentally ill people remain incarcerated in penal settings or living on the fringe of society. Over a career of twenty years in UK psychiatry, I have seen provision move from a hospital to a community model, leading to increased defensive and split practices (e.g. early intervention, crisis/home/in patient treatment, assertive outreach, rehabilitation and recovery etc).
Darwin’s survival of the fittest is evidenced through adaptation over several generations, but in mental health, adaptation must be achieved within a single lifetime, as individual circumstances are unique. How, when confronted with the plethora of interventions, can we enable mentally ill individuals, carers and professionals to find the appropriate combination?
I argue that professional splits increase defensive, mindless, practices (the quest for structure and function alienates us from the art of minding). Mental and social health call for minding others and ourselves. From Socrates’ questioning, Plato’s pursuit of supreme knowledge through dialogue, the antinomies of Kant, the Hegelian triad of thesis/ antithesis/ synthesis, we have struggled for constructive dialogue.
The Median Group, pioneered by the late Pat de Maré, offers a forum for ‘impersonal fellowship’. Through confronting idiosyncratic views, we can address stigma and splitting, thereby promoting healthier dialogue with each other and within ourselves, essential for healing.
“To be truly mindful of others, we have to reach a state of ‘no mind.’”
Yoganathan, N. Dr. Convenor of Median Groups, Group Analytic Society, London;
Consultant Psychiatrist, St Mary’s Hospital, Isle of Wight PCT NHS Trust
[email protected]; [email protected]
Human beings have survived millennia with diverse perceptions of mental illness: from imbalance in humidity of the brain (Hippocrates) or of the humours (Galen), through religious or evil possession, to the socio-dynamics of asylums, psycho-dynamics (structure of the mind) and latterly neuro-psycho-pharmacological and cognitive/behavioural understanding (function of the mind).
Economic-socio-political ideals have led to closure of large asylums in most of the industrialised nations. Although these changes have brought more humane, and more scientifically measurable, treatments, a large number of vulnerable, mentally ill people remain incarcerated in penal settings or living on the fringe of society. Over a career of twenty years in UK psychiatry, I have seen provision move from a hospital to a community model, leading to increased defensive and split practices (e.g. early intervention, crisis/home/in patient treatment, assertive outreach, rehabilitation and recovery etc).
Darwin’s survival of the fittest is evidenced through adaptation over several generations, but in mental health, adaptation must be achieved within a single lifetime, as individual circumstances are unique. How, when confronted with the plethora of interventions, can we enable mentally ill individuals, carers and professionals to find the appropriate combination?
I argue that professional splits increase defensive, mindless, practices (the quest for structure and function alienates us from the art of minding). Mental and social health call for minding others and ourselves. From Socrates’ questioning, Plato’s pursuit of supreme knowledge through dialogue, the antinomies of Kant, the Hegelian triad of thesis/ antithesis/ synthesis, we have struggled for constructive dialogue.
The Median Group, pioneered by the late Pat de Maré, offers a forum for ‘impersonal fellowship’. Through confronting idiosyncratic views, we can address stigma and splitting, thereby promoting healthier dialogue with each other and within ourselves, essential for healing.
“To be truly mindful of others, we have to reach a state of ‘no mind.’”
World Congress of Mental Health, Athens September 2009
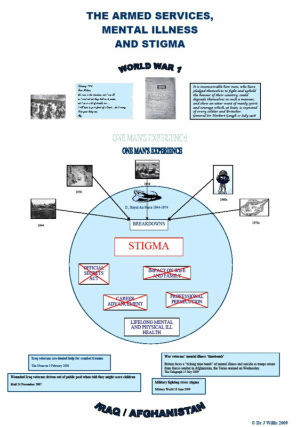
THE ARMED SERVICES, MENTAL ILLNESS AND STIGMA
Dr Jenny Willis
In order to explore institutional and public stigmatisation of mental illness, I present a case study of my father, now in his eighties, a retired officer of the Royal Air Force, whose mental health has been destroyed for the last fifty years by his professional duties. I shall begin by recognising that, had he lived in his father’s generation, he may not have reached this age. I shall use video and photographic images to recall the treatment of those suffering from what was variously described as shell shock, lack of moral fibre and neurasthenia, according to the victim’s social status, and examine the underlying stigma which determined the military and public response.
Returning to my father, I shall outline the nature of his work at the height of the Cold War, resulting in his breakdowns over a period of fifteen years, the medical treatment he received from the RAF, and the impact this had on his career. Added to the stigmatisation both he and the whole family suffered, his wife and children were secondary victims of the condition that was inadequately treated. I shall describe the reality of living with a person suffering from PTSD and the repercussions it has had on my own health.
Have military and public attitudes towards mental illness changed since then? Recent publicity surrounding those returning from active service in Iraq and Afghanistan might indicate progress, but first-hand reports from Service personnel suffering from PTSD tell a different story. The response of some local residents to a rehabilitation centre at Hedley Court reveals deep-seated prejudice.
I conclude that there is still much to be done to challenge institutional and public attitudes towards mental illness. My own contribution is through work with my partner, a Consultant Psychiatrist, in engaging professionals, sufferers and carers in dialogue.
Dr Jenny Willis
In order to explore institutional and public stigmatisation of mental illness, I present a case study of my father, now in his eighties, a retired officer of the Royal Air Force, whose mental health has been destroyed for the last fifty years by his professional duties. I shall begin by recognising that, had he lived in his father’s generation, he may not have reached this age. I shall use video and photographic images to recall the treatment of those suffering from what was variously described as shell shock, lack of moral fibre and neurasthenia, according to the victim’s social status, and examine the underlying stigma which determined the military and public response.
Returning to my father, I shall outline the nature of his work at the height of the Cold War, resulting in his breakdowns over a period of fifteen years, the medical treatment he received from the RAF, and the impact this had on his career. Added to the stigmatisation both he and the whole family suffered, his wife and children were secondary victims of the condition that was inadequately treated. I shall describe the reality of living with a person suffering from PTSD and the repercussions it has had on my own health.
Have military and public attitudes towards mental illness changed since then? Recent publicity surrounding those returning from active service in Iraq and Afghanistan might indicate progress, but first-hand reports from Service personnel suffering from PTSD tell a different story. The response of some local residents to a rehabilitation centre at Hedley Court reveals deep-seated prejudice.
I conclude that there is still much to be done to challenge institutional and public attitudes towards mental illness. My own contribution is through work with my partner, a Consultant Psychiatrist, in engaging professionals, sufferers and carers in dialogue.
Institute of Psychiatry, London
January 2009, The Dialectic of Stigma
Article & Poster session, Dr N Yoganathan & Dr J Willis
THE DIALECTIC OF STIGMA
Aim
The aim of this article is to provide a personal account of one psychiatrist’s approach to the complex issue of stigma in mental illness.
I have practised in the field of psychiatry since 1985, in both the NHS and independent sectors and currently work as a Consultant Psychiatrist for a Trust in the south-east of England. My co-author is an academic in the field of education.
Compliance and Stigma in Mental Illness
Compliance with treatment is paramount to recovery/stabilisation but adherence to treatment, particularly when it involves oral medication, is difficult to sustain. In respect of general medical conditions, the consensus is that compliance can range from 20% to 80%, dependent upon the condition and the level of recovery. The consequence of non-compliance is greater suffering, usually for the individual. However, when the condition is psychiatric in nature, repercussions may be far wider reaching.
A major contributory factor to non-compliance is the concept of ‘stigma’: a person’s subjective, negative response to the ailment. This, in turn, reinforces previously held assumptions and prejudices founded in limited knowledge and understanding of the condition. A hightened sense of stigma surrounds psychiatric conditions, exacerbated by aetiological ambiguity (nature vs. nurture) and therapeutic conflicts (drugs vs. psychological methods).
In order to break down the adverse impact of stigma in mental illness, The Royal College of Psychiatrists, together with the Department of Health, conducted a five-year anti-stigma campaign between 1998 and 2003. Large scale population surveys were conducted into public attitudes towards specific forms of mental illness (RCP November 2003). To complement them, day conferences were held at the Royal Society of Medicine. These activities sought to identify the forms and perpetrators of stigma, in preparation for a long-term process of change. As a participant at one of these conferences, I was left with a sense of helplessness in the face of public attitudes. Entrenched beliefs and attitudes often take decades or even centuries to change: for instance, readers may be surprised to learn that it was only in 1992 that the Roman Catholic Church formally accepted that the earth is round. Could we afford to wait this long to eradicate stigma from mental illness? My sense of helplessness against public attitudes was accompanied by a strong recognition that stigma must be addressed at the level of the individual if it is to be confronted effectively.
Patient choice and responsibility
Meanwhile, at the turn of the millennium, there had been a major change in medical practice, influenced partly by human rights legislation, and partly by the growth of information technology and the web. Patients’ choice and recognition of their rights are now integral to their treatment. This approach required immediate action, and at the individual rather than societal level.
Towards the end of the anti-stigma campaign, The Guardian published an article by Mark Radcliffe entitled Word Power: Can people with mental health problems take the sting out of stigma by reclaiming pejoratives? (Guardian 16 July 2003) This article reiterated the difficulties faced by carers and users in their struggle against stigma associated with mental illness, focusing on the pejorative use of language. In response, I wrote to the Guardian, emphasising the need to address stigma at the level of the individual, and commending median group as a vehicle for achieving this. My views were sufficiently persuasive for the Guardian to publish my contention that
it is naïve to believe that throwing large sums of money at a ‘problem’ will change attitudes that have become part of our culture over hundreds of years. We cannot realistically expect to undo the common pejorative use of terminology: it is an unconscious expression of the anxieties and confusion felt by those in power, an attempt to justify or rationalise certain human behaviours that may have more complex and uncomfortable causes. (Guardian 23 July 2003)
I went on to outline my ow approach
to encourage my patients to address aspects of stigma as an essential part of their treatment. I believe that the most
difficult stigma to overcome is one’s own, and I address this through education and, most importantly, in a group forum. A well-run group will provide aforum in w hich the pejorative use of language can be demystified, leading to true individual empowerment. (ibid)
Didactic vs dialectic
How did I come to this stance? During the early stages of my training, there was an emphasis on accurate diagnosis, based on history, examination and investigations. This led to scientific understanding of the condition(s) and to the planning and execution of appropriate treatments. A major turning point came for me when I became co-facilitator of a therapeutic group in 1988-1991. This group experience highlighted the art of psychiatry, particularly when trying to understand psychiatric conditions beyond their diagnoses. Consequently, I undertook further training in group work, leading to my qualification as a Convenor of Median Groups and a full member of the Group Analytic Society (London). (Hegelian principles and median groups, Pat de M)
Since my initial experience of dialectical thinking, I have incorporated this in my day-to-day work. Additionally, it has led me to devise a series of workshops aimed at users, carers and fellow professionals, to confront ‘stigma’.
References Radcliffe, M, 16 July 2003 Word Power, The Guardian
Royal College of Psychiatrists November 2003 Stigmatisation of people with mental Illness
Yoganthan, N, 23 July 2003, Battle of Words, The Guardian
Article & Poster session, Dr N Yoganathan & Dr J Willis
THE DIALECTIC OF STIGMA
Aim
The aim of this article is to provide a personal account of one psychiatrist’s approach to the complex issue of stigma in mental illness.
I have practised in the field of psychiatry since 1985, in both the NHS and independent sectors and currently work as a Consultant Psychiatrist for a Trust in the south-east of England. My co-author is an academic in the field of education.
Compliance and Stigma in Mental Illness
Compliance with treatment is paramount to recovery/stabilisation but adherence to treatment, particularly when it involves oral medication, is difficult to sustain. In respect of general medical conditions, the consensus is that compliance can range from 20% to 80%, dependent upon the condition and the level of recovery. The consequence of non-compliance is greater suffering, usually for the individual. However, when the condition is psychiatric in nature, repercussions may be far wider reaching.
A major contributory factor to non-compliance is the concept of ‘stigma’: a person’s subjective, negative response to the ailment. This, in turn, reinforces previously held assumptions and prejudices founded in limited knowledge and understanding of the condition. A hightened sense of stigma surrounds psychiatric conditions, exacerbated by aetiological ambiguity (nature vs. nurture) and therapeutic conflicts (drugs vs. psychological methods).
In order to break down the adverse impact of stigma in mental illness, The Royal College of Psychiatrists, together with the Department of Health, conducted a five-year anti-stigma campaign between 1998 and 2003. Large scale population surveys were conducted into public attitudes towards specific forms of mental illness (RCP November 2003). To complement them, day conferences were held at the Royal Society of Medicine. These activities sought to identify the forms and perpetrators of stigma, in preparation for a long-term process of change. As a participant at one of these conferences, I was left with a sense of helplessness in the face of public attitudes. Entrenched beliefs and attitudes often take decades or even centuries to change: for instance, readers may be surprised to learn that it was only in 1992 that the Roman Catholic Church formally accepted that the earth is round. Could we afford to wait this long to eradicate stigma from mental illness? My sense of helplessness against public attitudes was accompanied by a strong recognition that stigma must be addressed at the level of the individual if it is to be confronted effectively.
Patient choice and responsibility
Meanwhile, at the turn of the millennium, there had been a major change in medical practice, influenced partly by human rights legislation, and partly by the growth of information technology and the web. Patients’ choice and recognition of their rights are now integral to their treatment. This approach required immediate action, and at the individual rather than societal level.
Towards the end of the anti-stigma campaign, The Guardian published an article by Mark Radcliffe entitled Word Power: Can people with mental health problems take the sting out of stigma by reclaiming pejoratives? (Guardian 16 July 2003) This article reiterated the difficulties faced by carers and users in their struggle against stigma associated with mental illness, focusing on the pejorative use of language. In response, I wrote to the Guardian, emphasising the need to address stigma at the level of the individual, and commending median group as a vehicle for achieving this. My views were sufficiently persuasive for the Guardian to publish my contention that
it is naïve to believe that throwing large sums of money at a ‘problem’ will change attitudes that have become part of our culture over hundreds of years. We cannot realistically expect to undo the common pejorative use of terminology: it is an unconscious expression of the anxieties and confusion felt by those in power, an attempt to justify or rationalise certain human behaviours that may have more complex and uncomfortable causes. (Guardian 23 July 2003)
I went on to outline my ow approach
to encourage my patients to address aspects of stigma as an essential part of their treatment. I believe that the most
difficult stigma to overcome is one’s own, and I address this through education and, most importantly, in a group forum. A well-run group will provide aforum in w hich the pejorative use of language can be demystified, leading to true individual empowerment. (ibid)
Didactic vs dialectic
How did I come to this stance? During the early stages of my training, there was an emphasis on accurate diagnosis, based on history, examination and investigations. This led to scientific understanding of the condition(s) and to the planning and execution of appropriate treatments. A major turning point came for me when I became co-facilitator of a therapeutic group in 1988-1991. This group experience highlighted the art of psychiatry, particularly when trying to understand psychiatric conditions beyond their diagnoses. Consequently, I undertook further training in group work, leading to my qualification as a Convenor of Median Groups and a full member of the Group Analytic Society (London). (Hegelian principles and median groups, Pat de M)
Since my initial experience of dialectical thinking, I have incorporated this in my day-to-day work. Additionally, it has led me to devise a series of workshops aimed at users, carers and fellow professionals, to confront ‘stigma’.
References Radcliffe, M, 16 July 2003 Word Power, The Guardian
Royal College of Psychiatrists November 2003 Stigmatisation of people with mental Illness
Yoganthan, N, 23 July 2003, Battle of Words, The Guardian

Opening session 23 January 2009

World Federation for Mental Health Congress Cape Town October 2011
Mental health in the
21st century: confronting uncomfortable lessons from the industrialised
world
Dr N Yoganathan & Dr J Willis
Mental Health services in the industrialised countries have been going through major changes since the late 20th century. Closure of asylums and ‘in-patient’ facilities are being replaced by various alternatives and a plethora of therapies, bringing with them new terminology, professional roles and titles. Yet, despite significant advances in scientific understanding, increasing professional manpower and more effective medicines, the number of people with mental health problems who are languishing in the penal system and on the fringes of society is soaring dramatically. Notwithstanding international, national and local campaigns, stigma associated with mental illness remains rampant. Stresses on mental health professionals are also on the increase.
As two professionals working throughout this period, one from a medical and group analytical background, the other a higher education researcher in psychosocial/linguistic domains, we believe that 21st century psychiatric care in the ‘developed world’ is riddled with professional splits, short-term ‘solutions’ and ambiguous language, masking the despair experienced by all involved. Emphasis on ‘evidence-based’ practice inevitably results in approaches that are impersonal and divisive, tantamount to simplistic Oedipal and pre-Oedipal processes.
In Hong Kong (2007) and Athens (2009), we addressed aspects of stigma and defensive, mindless, practices in psychiatric care, and called for a dialogue between evidence- and tradition-based practice to minimise professional conflicts and mutual stress.
Our proposed workshop, based on Median Group (post-Oedipal) principles of dialogue, draws from Socrates’ questioning, Plato’s pursuit of supreme knowledge through dialogue, the antinomies of Kant, and the Hegelian triad of thesis/ antithesis/ synthesis. It offers an opportunity to confront individual perceptions, values and prejudices. Through a process of pre- and post-workshop reflection and feedback, we aim to capture shifts in individual and collective attitudes and understanding, and (hopefully) learn some valuable lessons that will help shape the future of mental health care in Africa and beyond.
Dr N Yoganathan & Dr J Willis
Mental Health services in the industrialised countries have been going through major changes since the late 20th century. Closure of asylums and ‘in-patient’ facilities are being replaced by various alternatives and a plethora of therapies, bringing with them new terminology, professional roles and titles. Yet, despite significant advances in scientific understanding, increasing professional manpower and more effective medicines, the number of people with mental health problems who are languishing in the penal system and on the fringes of society is soaring dramatically. Notwithstanding international, national and local campaigns, stigma associated with mental illness remains rampant. Stresses on mental health professionals are also on the increase.
As two professionals working throughout this period, one from a medical and group analytical background, the other a higher education researcher in psychosocial/linguistic domains, we believe that 21st century psychiatric care in the ‘developed world’ is riddled with professional splits, short-term ‘solutions’ and ambiguous language, masking the despair experienced by all involved. Emphasis on ‘evidence-based’ practice inevitably results in approaches that are impersonal and divisive, tantamount to simplistic Oedipal and pre-Oedipal processes.
In Hong Kong (2007) and Athens (2009), we addressed aspects of stigma and defensive, mindless, practices in psychiatric care, and called for a dialogue between evidence- and tradition-based practice to minimise professional conflicts and mutual stress.
Our proposed workshop, based on Median Group (post-Oedipal) principles of dialogue, draws from Socrates’ questioning, Plato’s pursuit of supreme knowledge through dialogue, the antinomies of Kant, and the Hegelian triad of thesis/ antithesis/ synthesis. It offers an opportunity to confront individual perceptions, values and prejudices. Through a process of pre- and post-workshop reflection and feedback, we aim to capture shifts in individual and collective attitudes and understanding, and (hopefully) learn some valuable lessons that will help shape the future of mental health care in Africa and beyond.
Related journal and videos

World Congress of the World Federation for Mental Health: Cape ...
► 1:16► 1:16
www.youtube.com/watch?v=r-ncXDFQTH020 Oct 2011 - 1 min - Uploaded by amandabmahony
World Congress of the World Federation for Mental Health: Cape Town, 2011. Amanda Mahony. Subscribe ...
More videos for cape town world federation for mental health »
► 1:16► 1:16
www.youtube.com/watch?v=r-ncXDFQTH020 Oct 2011 - 1 min - Uploaded by amandabmahony
World Congress of the World Federation for Mental Health: Cape Town, 2011. Amanda Mahony. Subscribe ...
More videos for cape town world federation for mental health »
UK EVENTS
Staff Development, Bedfordshire, 2005

Dr N Yoganathan & Dr J Willis
Promoting Social Inclusion through Vocational Rehabilitation ...
www.advancingpractice.co.uk/journal%20edition%204(3).pdf
File Format: PDF/Adobe Acrobat - Quick View
by J Butler - Related articles
2 Jun 2008 – Volume 4: Number 3 (Autumn 2007). ISSN: 1743-1611 (On-line). 89. Editorial Group: Advancing Practice in Bedfordshire. John Butler ...
Promoting Social Inclusion through Vocational Rehabilitation ...
www.advancingpractice.co.uk/journal%20edition%204(3).pdf
File Format: PDF/Adobe Acrobat - Quick View
by J Butler - Related articles
2 Jun 2008 – Volume 4: Number 3 (Autumn 2007). ISSN: 1743-1611 (On-line). 89. Editorial Group: Advancing Practice in Bedfordshire. John Butler ...
Mental Health Congress, HSJ Nursing Times
CBI Conference Centre, 27-28 November 2012
Panelist: Dr N Yoganathan
Workshop: Dr N Yoganathan & Dr J Willis
Panelist: Dr N Yoganathan
Workshop: Dr N Yoganathan & Dr J Willis
